



Appointments
Request Appointment/Request Exam - After completing the respective forms, these requests will be processed by our services, and you will receive confirmation by email. The indications about the Agreements (Insurance/Subsystem) are merely informative, please request confirmation in the "Observations" field.
Schedule Appointment/Exam myHPA - By accessing myHPA Saúde you can make the appointment in real time, directly on the Doctor's schedule according to his availability.
You can also contact us at +351 282 420 400 Algarve | +351 269 630 370 Alentejo | +351 291 003 300 Madeira
Phone booking/service hours:
Monday to Friday: 8:00 AM to 7:00 PM, Saturday: 8:00 AM to 5:00 PM Sunday and Holidays: Closed
(National landline)
Your request has been successfully received. We will confirm your appointment shortly.
Download myHPA Saúde:


HPA Health Group Newsletter:
Subscribe and stay up to date with all the news!
Dr. Felix Bartzsch
Gynaecologist/Obstetrician
Specialist in Gynaecology and Breast Oncology
Specialist in Urogynaecology and Laparoscopic Gynaecology Surgery

Dr.ª Carmen Klink
Gynaecologist/Obstetrician
Especialista em Senologia
e Ginecologia Oncológica
Especialista em Uroginecologia e Cirurgia Ginecológica Laparoscópica

Laparoscopic Hysterectomy
HPA Magazine 13
With this article, we want to present the procedure of hysterectomy in general, and explain in detail the laparoscopic approach. Furthermore, we want to describe the indications, possible complications, advantages and disadvantages of this minimal-invasive procedure.
The word hysterectomy has a Greek root and means removal of the womb. The uterus can be removed in its entirety (total hysterectomy) or only partially (subtotal or supracervical hysterectomy). In these cases, the cervix is preserved. When removal of the ovaries and/or fallopian tubes is performed simultaneously, the intervention is called hysterectomy with adnexectomy (respectively oophorectomy or salpingectomy).
A hysterectomy can be performed in various ways depending on the diagnosis, the indication, the patient's request and the surgical experience of the gynecologist. It is always an individual decision, taken mutually between the well-informed patient and the doctor.
Hysterectomies are one of the most frequently performed gynecological surgeries, for example with around 600,000 hysterectomies performed annually in the United States, 66% of which are abdominal.
HISTORY
The first attempts to remove the uterus date back to the 1st Century and up until the 18th Century the women who underwent a hysterectomy seldom survived.
The first successful abdominal hysterectomy was performed in 1853 and vaginally in 1861. Since then, these procedures were constantly developed and improved, with the first (key-hole) laparoscopic hysterectomy taking place in Pennsylvania in 1988. Other laparoscopic variants have since then evolved such as the radical and ultra-radical oncologic surgical procedures performed today.
METHODS
A hysterectomy can be performed vaginally, abdominally, laparoscopically, vaginally laparoscopically assisted, single-incision laparoscopic (SILS), natural orifice endoscopic transluminal (NOTES), and robotic.
INDICATIONS
Indications for a hysterectomy are diverse, among them: fibroids (benign lumps of the womb), abnormal bleeding, uterine prolapse, infection, inflammation and pain, endometriosis, cancer, pre-malignant lesions and the patient’s request.
LAPAROSCOPIC HYSTERECTOMIES
Using the laparoscopic technique, a hysterectomy can be performed mainly as follows: total laparoscopic hysterectomy (TLH), supracervical/subtotal laparoscopic hysterectomy (LASH) and laparoscopic assisted vaginal hysterectomy (LAVH).
For any laparoscopic procedure, access to the abdominal cavity is necessary in order to position the camera and surgical instruments. This is accomplished through small holes of 5 to 10 mm. For the specialist to visualize the area, it is necessary to insufflate the abdomen with CO2 (carbon dioxide), which at the end of surgery is again removed.
Total Laparoscopic Hysterectomy (TLH). This is a technique, where the uterus is completely separated from the blood vessels and its supporting structures, exclusively via laparoscopy. Usually three to four puncture holes are required in the abdomen. The uterus is then removed via the vagina. With this method large scars are avoided, the risk of infections is very low, recovery is usually much faster, hospitalization and the return to daily activities much shorter, compared to open abdominal surgery. Disadvantages include the slightly increased risk of urogenital lesions such as bladder and ureter injuries and a slightly longer operative time. Usually the patient is discharged on the second postoperative day and practically has no need of analgesics.
Supracervical/subtotal Laparoscopic Hysterectomy (LASH). With this type of intervention, the uterus is not removed in its entirety; the cervix remains, allowing stability of the pelvic structures. This technique also requires three to four puncture holes through which special coagulation, cutting and clamping instruments are introduced. After preparation, the body of the uterus is separated from the cervix. By using a morcellator (“shredder”) * the uterus is removed via the abdominal cavity avoiding a large scar. The advantages and disadvantages are similar to the method used in a total laparoscopic hysterectomy.
Laparoscopic assisted Vaginal Hysterectomy (LAVH). This surgery is the combination of a vaginal and laparoscopic approach. The indication for this procedure is when a vaginal hysterectomy can be performed, but at the same time intraabdominal pathologies exist, for example of the ovaries or fallopian tubes. After solving the intraabdominal pathology, the uterus is removed via the vagina. In addition to the advantages described previously, this method implies a lower risk of urogenital lesions and operating time is also reduced.
In general, laparoscopic techniques have a very limited indication for patients with cardiopulmonary limitations, as abdominal insufflation with CO 2 may worsen these dysfunctions during surgery, causing relevant intra-operative complications. On the other hand, they are strongly indicated especially in obese patients, as they avoid problems related to healing, infections and prolonged hospitalization.
An essential factor for any type of surgery is the surgeon's experience and skill, as well as how often the surgeon performs these surgeries.
The deciding factors for the different laparoscopic techniques are: size and position of the uterus, its accessibility, the condition to be treated, post-caesarean section or other surgeries, parity (number of deliveries), overweight and other personal history.
A hysterectomy irreversibly ends the possibility of a future pregnancy. Menstruation disappears because the inner layer of the uterus (endometrium) is removed. On the other hand, in a subtotal hysterectomy, “spotting” may occasionally occur due to the fact that in the cervix some endometrial cells may persist and react to the hormonal cycle.
It is important to mention, that removal of the uterus or part of it does not imply that the woman enters into menopause. Menopause is directly linked to ovarian failure or removal.
All studies conducted so far, clearly show a high satisfaction of patients who underwent a hysterectomy, regardless of the access route. The mere fact that menstruation is over, and no contraception is needed, increases the patient’s quality of life significantly. There is no convincing indication that this surgery causes sexual or psychic dysfunction. On the other hand, there are women who suffer from the “loss” of their womb, expressing that they no longer feel like “a complete woman”.
According to the Maryland Women's Health Study, 85% of women indicated, after a hysterectomy, an increased frequency of sexual intercourse, less pain during sex (dyspareunia), increased libido and orgasms, as well as fewer problems such as vaginal dryness.
Another much discussed topic is the association of a hysterectomy with urinary incontinence. It is not clear if the surgery itself or other preoperative factors determine the likelihood of posthysterectomy urinary incontinence, as the appearance of incontinence increases in all women over time.
COMPLICATIONS
Complications can be classified as intraoperative (during surgery) and postoperative. An analysis of the 103,000 hysterectomies performed in Germany in 2012 revealed a 1.4% (intraoperative) and 4% (postoperative) complication rate. The percentage of intraoperatory switch from vaginal/laparoscopic to abdominal approach is around 2%. Intraoperative complications with bladder injuries have a direct correlation with previous cesarean sections as well as the size of the uterus. ureter injuries is less than 1%. Urogenital fistulas or prolapse varies between the various surgical approaches.
Current data is incongruent regarding the risk of prolapse recurrence following a hysterectomy, regardless of access route. Blood vessel lesions go up to 3% and lesions of the bowel up to 0.2%.
Postoperative complications include pneumonia (0.03%), cardiovascular complications (0.18%), thrombosis (0.02%) and pulmonary embolism (0.03%), as for any major laparoscopic surgery.
ALTERNATIVES
There are many indications for alternative treatments of a hysterectomy, whether conservative or drug-induced. For uterine fibroids an alternative may be embolization or isolated removal of the fibroid. Targeted pelvic-strengthening physiotherapy can in some cases improve the symptoms of a prolapse.
Concluding, it can be said, that currently a hysterectomy is a very safe, effective procedure with a low complication rate, permitting a significant increase in the women's quality of life. Among the possible access routes, vaginal and laparoscopic access should be privileged options.
LAPAROSCOPIC SUPRACERVICAL HYSTERECTOMY (LASH)






Fotografias · Photos: Gindual© Lda
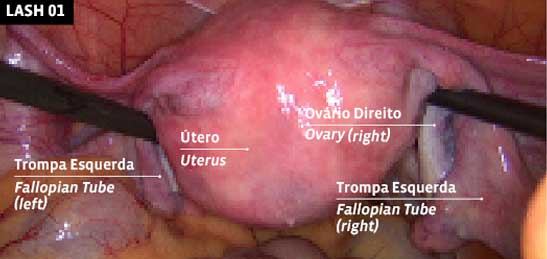
LASH 01
UTERUS
Initial condition: uterus with fallopian tubes and ovaries.
LASH 02
REMOVAL OF FALLOPIAN TUBES
Removal of left fallopian tube.
LASH 03
UTERUS WITHOUT FALLOPIAN TUBES
Condition after removal
of fallopian tubes.
LASH 04
UTERUS REMOVED
Uterus separated from the cervix.
LASH 05
SUTURE
Peritoneum suture.
LASH 06
MORCELLATION
Morcellation of the uterus.
LASH 07
FINAL
Final condition suture after removal of the uterus and tubes. Both ovaries preserved.
CONTINUE ENJOYING LIFE
Although I work in a medicial centre, it is very easy to ignore your own health when there are several things going on but nothing you can put your finger on, say Gail. My symptoms were very nonspecific and varied. Luckily at my first consultation with Dr Carmen Klink my diagnosis was made with the help of a simple and painless vaginal ultrasound done at the first consultation. I had a further consultation to discuss the best treatment for me as I did have quite a few things diagnosed and i needed a complete hysterectomy. My laparoscopy was then scheduled with Dr Carmen and Dr Felix.
The procedure was fully explained to me, and although it involves a general anesthetic, the modern technique means no large tummy cuts or long recovery period. My stay in hospital was three days and I felt fine after the first day, and was more than ready to go home on the third day as planned. I recovered really quickly, only have 3 very tiny scars that you can hardly see, and was back at work within a fortnight of the operation. I feel great, my symptoms have all disappeared and a follow up consultation showed that all had healed well. My mind is at rest now and I can get on and enjoy life again.

INNOVATE
Although I work in a medicial centre, it is very easy to ignore your own health when there are several things going on but nothing you can put your finger on, say Gail. My symptoms were very nonspecific and varied. Luckily at my first consultation with Dr Carmen Klink my diagnosis was made with the help of a simple and painless vaginal ultrasound done at the first consultation. I had a further consultation to discuss the best treatment for me as I did have quite a few things diagnosed and i needed a complete hysterectomy. My laparoscopy was then scheduled with Dr Carmen and Dr Felix. The procedure was fully explained to me, and although it involves a general anesthetic, the modern technique means no large tummy cuts or long recovery period. My stay in hospital was three days and I felt fine after the first day, and was more than ready to go home on the third day as planned. I recovered really quickly, only have 3 very tiny scars that you can hardly see, and was back at work within a fortnight of the operation. I feel great, my symptoms have all disappeared and a follow up consultation showed that all had healed well. My mind is at rest now and I can get on and enjoy life again.
Carlpos Borlido · Theater Nurse, Responsible for the Operating Theater of the HPA in Alvor
