Appointments
Request Appointment/Request Exam - After completing the respective forms, these requests will be processed by our services, and you will receive confirmation by email. The indications about the Agreements (Insurance/Subsystem) are merely informative, please request confirmation in the "Observations" field.
Schedule Appointment/Exam myHPA - By accessing myHPA Saúde you can make the appointment in real time, directly on the Doctor's schedule according to his availability.
You can also contact us at +351 282 420 400 Algarve | +351 269 630 370 Alentejo | +351 291 003 300 Madeira
Phone booking/service hours:
Monday to Friday: 8:00 AM to 7:00 PM, Saturday: 8:00 AM to 5:00 PM Sunday and Holidays: Closed
(National landline)
Your request has been successfully received. We will confirm your appointment shortly.
Download myHPA Saúde:


HPA Health Group Newsletter:
Subscribe and stay up to date with all the news!
Dr. João Costa
Surgical pathologist
The role of Surgical Pathology in detecting Lynch Syndrome
HPA Magazine 24 // 2025
Lynch syndrome is a hereditary cancer predisposition syndrome associated with germline alterations involving the MLH1, PMS2, MSH2, MSH6 and EPCAM genes (among others), and is associated with a high risk of several neoplasms, mainly colorectal and endometrial carcinomas. It is also associated with an increased risk of ovarian, urothelial, gastric, small intestine, pancreatic and hepatobiliary tract carcinomas, central nervous system and skin neoplasms, among others. It is estimated that approximately 1 in 450 people have Lynch syndrome and that only about 5% of these people are diagnosed. The cumulative lifetime risk of colorectal and endometrial carcinomas in patients with this syndrome is approximately 10-80% and 21-71%, respectively (depending on the altered gene), and it is estimated that 3-5% of colorectal carcinomas and 2-6% of endometrial carcinomas are associated with this syndrome. Detection of Lynch syndrome is of the utmost importance, not only because patients benefit from adapted surveillance protocols and preventive therapies, but also to detect other asymptomatic carriers in the families of these patients.
The MLH1, PMS2, MSH2, and MSH6 genes are involved in the mismatch repair mechanism. This mechanism is responsible for repairing a specific type of error in DNA replication. Defects in this mechanism lead to the accumulation of these errors, especially in microsatellites (small repetitive sequences in DNA), leading to microsatellite instability.
This syndrome has an autosomal dominant inheritance pattern. The patient inherits an allele with the affected gene from one parent, but inactivation of the second allele is necessary for carcinogenesis to occur. Inactivation of the second allele can occur through several mechanisms, the most common being hypermethylation of the MLH1 promoter.
Clinical criteria for identifying patients with a high probability of Lynch syndrome (the Amsterdam, Bethesda, and modified Bethesda criteria, among others) fail to identify a significant number of patients, and, as such, new screening strategies are needed. Currently, the National Comprehensive Cancer Network, the European Society for Medical Oncology, and other international societies recommend universal screening of all cases of colorectal and endometrial carcinomas. The National Comprehensive Cancer Network also recommends considering screening for all sebaceous neoplasms, as well as all carcinomas of the small intestine, gastric, ovarian, urothelial, and adrenocortical carcinomas, and neoplasms of the central nervous system, regardless of age. This screening is performed by surgical pathologists using two methods: immunohistochemical study to detect proteins involved in the mismatch repair mechanism, or microsatellite instability testing, both of which are performed in tumour tissue. In addition to detecting patients at risk of having Lynch syndrome, this screening also provides additional information, with diagnostic (these techniques are used by surgical pathologists in the evaluation of neoplasms, for differential diagnosis purposes, and, in cases of endometrial carcinomas and some types of ovarian carcinomas, to carry out molecular classification using the algorithm based on The Cancer Genome Atlas), prognostic and theragnostic value (response to therapy with immune checkpoint inhibitors).
The immunohistochemical study detects the expression of proteins encoded by the MLH1, PMS2, MSH2 and MSH6 genes in the tumour tissue. In a test without alterations, the normal expression of all 4 proteins is detected, and it is very unlikely that there is a pathogenic alteration in one of the genes involved. In a test with alterations, one or more of the proteins was not detected and a pathogenic alteration of the gene(s) involved may be present, and subsequent tests are recommended to determine whether the patient has Lynch syndrome. The immunohistochemical study is cheaper, requires fewer resources, has better developed external quality control schemes, allows correlation with the morphological aspects of the tumour and the results allow a more targeted guidance for subsequent tests required for screening for Lynch syndrome. If combined loss of MSH2 and MSH6, or isolated losses of MSH6 and PMS2, is detected, the patient should be evaluated by Medical Genetics for screening for the syndrome. However, if there is a combined loss of the MLH1 and PMS2 proteins, in cases of colorectal carcinoma, the first step should be to test for hypermethylation of the MLH1 gene promoter and the BRAF V600E mutation, and in cases of endometrial carcinoma, to test solely for hypermethylation of the MLH1 gene promoter. If these tests are negative, the patient should be evaluated by Medical Genetics to screen for Lynch syndrome (the presence of hypermethylation of the MLH1 gene promoter and the BRAF V600E mutation is associated with a very low probability of the aforementioned syndrome).
Testing for microsatellite instability is performed by evaluating differences in the length of a set of microsatellites, either by polymerase chain reaction or by massive parallel sequencing. This test is more expensive, requires more resources, does not allow correlation with morphology, and the sensitivity of the different tests available varies depending on the type of cancer. Thus, microsatellite instability testing tends to be used in more specific contexts, namely, in situations in which the immunohistochemical study presents results that are difficult to interpret, in cases without loss of expression of the proteins involved in the mismatch repair mechanism in patients with a high probability of being carriers of Lynch syndrome, and in situations of contradictory results between the immunohistochemical study and the molecular study. In cases of tumours classified as having high microsatellite instability (MSI high) or indeterminate results, the patient should be evaluated by Medical Genetics to screen for Lynch syndrome. More than 90% of tumours in patients with Lynch syndrome present microsatellite instability/absence of immunoexpression of one or more proteins – if the clinical suspicion for this syndrome is high, germline mutation testing should be performed, even if the tumour is negative. The concordance rate between immunohistochemical testing and microsatellite instability testing is 95%, and one or the other modality may be chosen, depending on local resources. There is a false negative rate of 5-10% with immunohistochemical testing and 5-15% with microsatellite instability testing.
Unilabs has a large team of specialized pathologists, dedicated to different areas of expertise. The Surgical Pathology service offers high-quality histopathological and cytopathological evaluation of cytology specimens, biopsies and surgical specimens. It also has a highly specialized, multidisciplinary, Molecular Biology team, composed of physicians, biologists and qualified technicians, enabling us to provide more precise guidance in patient monitoring. Unilabs has available the immunohistochemical study to evaluate the proteins encoded by the MLH1, PMS2, MSH2 and MSH6 genes, and, through its partners, microsatellite instability testing, MLH1 gene promoter hypermethylation testing, BRAF V600E mutation testing and detection of changes in the MLH1, PMS2, MSH2 and MSH6 genes.
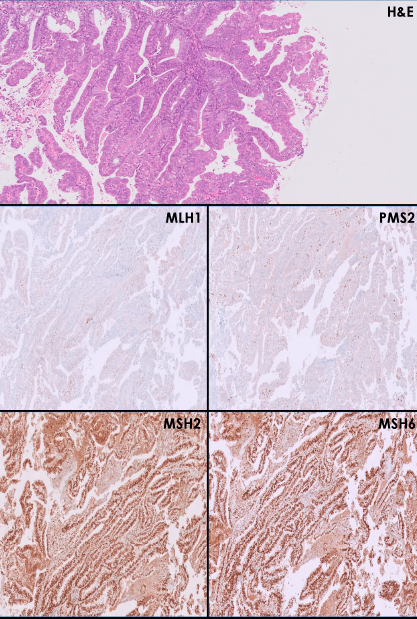
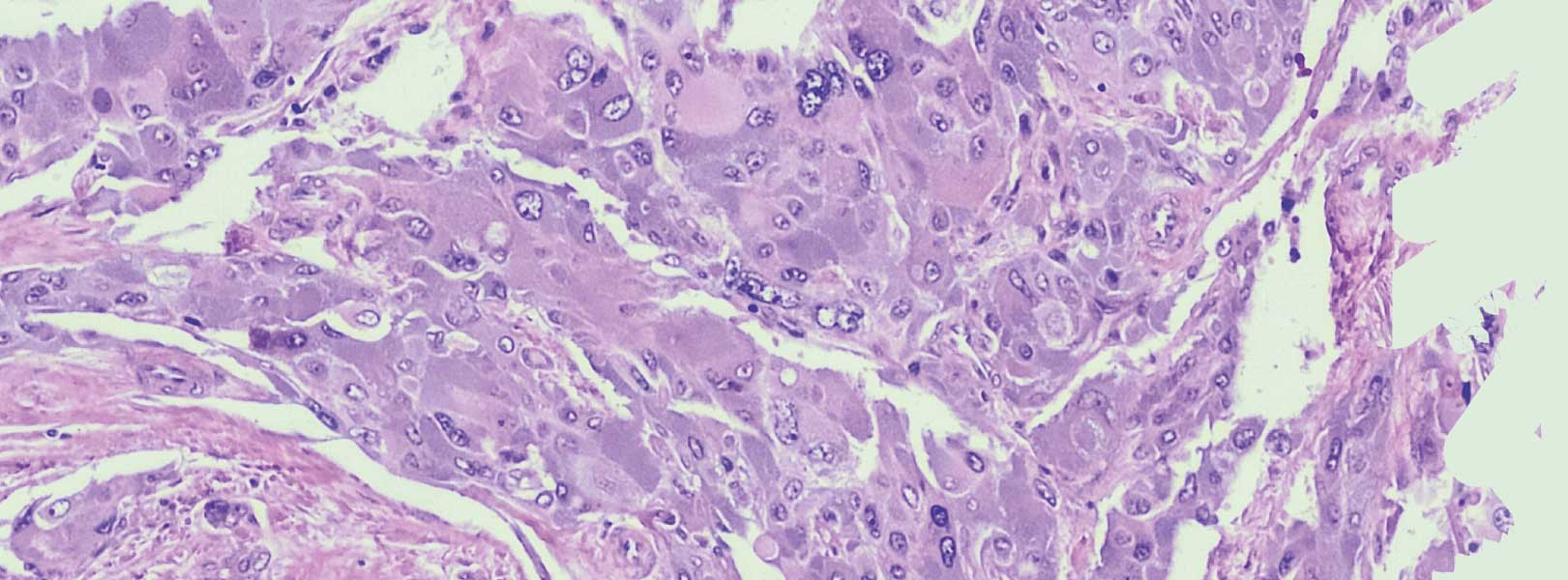
Figure 1:
A low-grade endometrial endometrioid carcinoma (well-differentiated – G1) with loss of expression of the MLH1 and PMS2 proteins and retained expression of the MSH2 and MSH6 proteins. This result is compatible with mismatch repair deficiency. In these cases, MLH1 gene promoter hypermethylation testing should be performed.