





Appointments
Request Appointment/Request Exam - After completing the respective forms, these requests will be processed by our services, and you will receive confirmation by email. The indications about the Agreements (Insurance/Subsystem) are merely informative, please request confirmation in the "Observations" field.
Schedule Appointment/Exam myHPA - By accessing myHPA Saúde you can make the appointment in real time, directly on the Doctor's schedule according to his availability.
You can also contact us at +351 282 420 400 Algarve | +351 269 630 370 Alentejo | +351 291 003 300 Madeira
Phone booking/service hours:
Monday to Friday: 8:00 AM to 7:00 PM, Saturday: 8:00 AM to 5:00 PM Sunday and Holidays: Closed
(National landline)
Your request has been successfully received. We will confirm your appointment shortly.
Download myHPA Saúde:


HPA Health Group Newsletter:
Subscribe and stay up to date with all the news!
Dra. Sílvia Vieira
Obstetrician Gynaecologist
Coordinator of the
Endometriosis Diagnosis
and Treatment Centre

Uterine fibroids:
Updates on epidemiology, diagnosis and risk factors
HPA Magazine 24 // 2025
Uterine fibroids are the most common benign tumours of the female genital tract, with a high clinical impact, responsible for significant gynaecological morbidity and the main cause of hysterectomy in women of reproductive age.

Definition and Histopathology
Uterine fibroids are monoclonal benign mesenchymal tumours originating from smooth muscle cells and fibroblasts of the myometrium. Histologically, fibroids show organized cellular proliferation and may undergo hyaline, cystic, haemorrhagic, or calcified degenerations.
Epidemiology
The true incidence of fibroids is underestimated due to a high proportion of asymptomatic cases. The estimated prevalence is between 20% and 40% in women of childbearing age, increasing to 70% to 80% by age 50. The incidence is 2 to 3 times higher in black women, who tend to have more symptomatic, voluminous, multiple lesions, and an earlier onset. The frequency tends to decrease with menopause.
Etiopathogenesis
The pathogenesis involves two main events:
1. Somatic mutations in normal myocytes leading to their transformation into altered cells.
2. Clonal growth of these altered cells under hormonal and growth factor stimulation.
Genetic, hormonal (particularly oestrogen and progesterone), environmental, and epigenetic factors are implicated.
Risk Factors
Several factors are associated with an increased risk of developing fibroids, including:
• Advanced reproductive age
• Early menarche
• Nulliparity
• Interval > 5 years since the last birth
• Vitamin D deficiency
• In utero exposure to diethylstilbestrol (DES)
• Exposure to endocrine disruptors (phthalates, BPA, PCBs, organochlorines)
• Chronic stress and major life events
Protective Factors
Studies suggest a protective effect of:
• Parity ≥ 3 births
• Advanced maternal age at first birth
• Short interval since the last birth
• Levonorgestrel intrauterine device (LNG-IUD)
• Medroxyprogesterone acetate
• Diet rich in fruits, vegetables, fish, and dairy products
• Regular physical exercise
• Type 2 diabetes mellitus
The association between smoking and a reduced risk of myomas, attributed to aromatase inhibition, remains controversial.
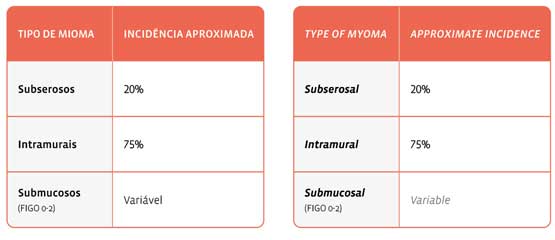
Classification and Location
Myomas can be classified according to their location as:
The classification of the International Federation of Gynaecology and Obstetrics (FIGO), together with the European Society for Gynaecological Endoscopy (ESGE), has been widely adopted for diagnostic and therapeutic standardization. This classification considers the degree of penetration of the myoma into the endometrial cavity and its relationship with the myometrial wall.
Clinical Manifestations
Symptoms vary according to the number, size, and location of the myomas. The most frequent symptoms include:
• Abnormal uterine bleeding (AUB)
• Pelvic or lower back pain
• Palpable abdominal mass
• Infertility and implantation failure
• Recurrent miscarriages
• Compressive symptoms (bladder and rectum)
Diagnosis
The diagnosis is based on clinical evaluation and complementary exams:
Clinical exam
• Bimanual palpation: enlarged, lumpy, hard-elastic uterus
• Speculum examination: may reveal myoma protruding through the cervical canal
Imaging exams
• Transvaginal Pelvic Ultrasound (TVUS): initial exam of choice, with high sensitivity for lesions ≥ 1 cm
• Transabdominal Ultrasound: complementary in cases of a large uterus
• Hysterosonography (HSN): useful for evaluating deformity of the endometrial cavity
• Magnetic Resonance Imaging (MRI): ideal for preoperative mapping, especially in multiple, submucosal, or degenerated myomas
• Diagnostic Hysteroscopy: indicated in cases of suspected intracavitary fibroids; allows diagnosis and treatment in the same procedure
Laboratory tests
• Measurement of lactic dehydrogenase (LDH) and isoenzymes can help in the differential diagnosis with sarcoma, although without sufficient specificity to exclude malignancy.
Final Considerations
Despite being benign, uterine fibroids have a significant impact on women's quality of life and reproductive health. Early diagnosis and appropriate classification are essential for therapeutic definition. Differentiation from malignant tumours such as sarcomas still represents a challenge, reinforcing the importance of individualized multidisciplinary evaluation.
